Liver Detoxification
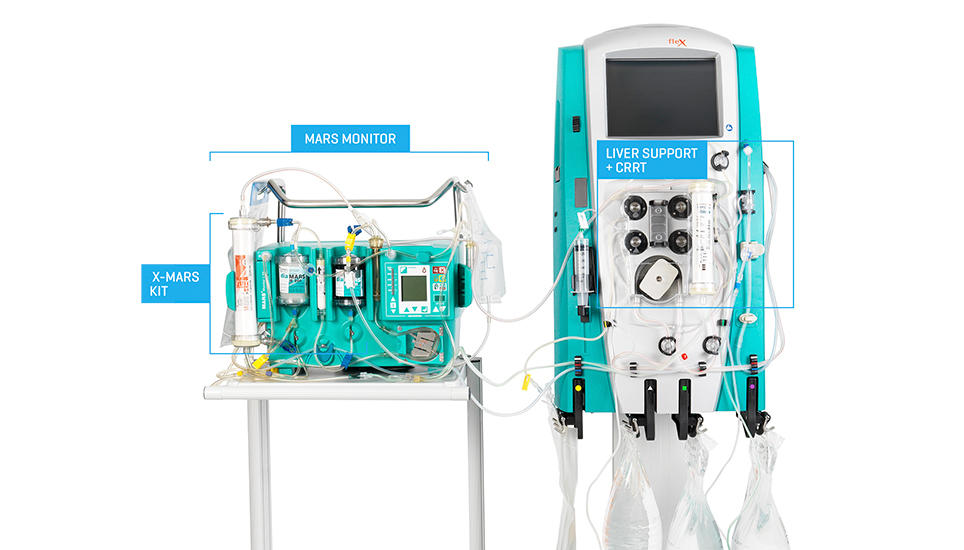
MARS + PRISMAFLEX: Joining forces for the treatment of drug overdose
Dual Powered. Single Purpose.
The MARS (Molecular Adsorbent Recirculating System) therapy works easily with your PRISMAFLEX System to support the removal of harmful drugs and poisons in combination with CRRT. Tap the blue buttons in the top left of the image below for more info.